In my last blog I talked about Benign Paroxysmal Positional Vertigo (BPPV) as being the most common form of dizziness and its characteristics. In this blog I will explain how it is diagnosed and some treatments.
Diagnosis
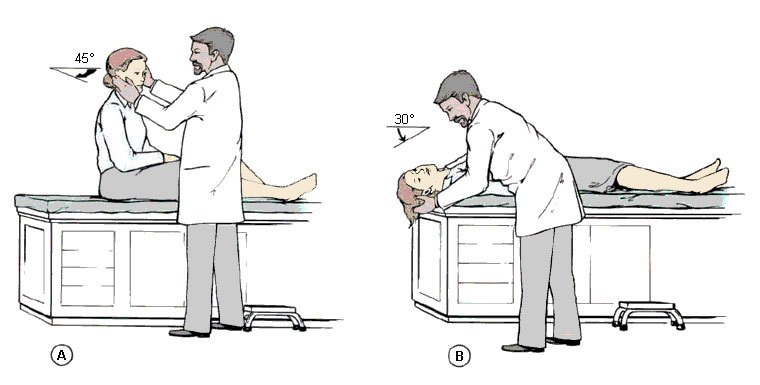
Once BPPV is suspected based on your case history; the clinician may decide to do the Dix-Hallpike to confirm. The Dix-Hallpike is performed by rotating the patient’s head by 45 degrees. The clinician then helps the patient lie backwards quickly dropping the head at approximately 20 degrees of extension. This extension is achieved by the clinician supporting the head as it hangs off the table. The clinician then observes the patient’s eyes for 45 seconds in this position. If a repetitive eye jump (nystagmus) occurs then it is considered positive for BPPV. If the patient feels dizzy without eye jumping (nystagmus) this is not considered positive for BPPV. Something else is causing the dizziness.
If nystagmus is observed repeat the maneuver 2 times to see if the response fatigues. Fatigues means the response will decrease every time the test is repeated. If the response fatigues it is confirmed the patient has BPPV. If the nystagmus response does not fatigue it suggests the cause is not inner ear related, could be brain or spine.
There are six possible types of BPPV and there are different treatments for each.
- Left posterior canal
- Right posterior canal
- Left superior canal
- Right superior canal
- Left lateral canal
- Right lateral canal
Treatment for Posterior Canal
This is the most common form of BPPV. You can use the Epley maneuver for treatment.
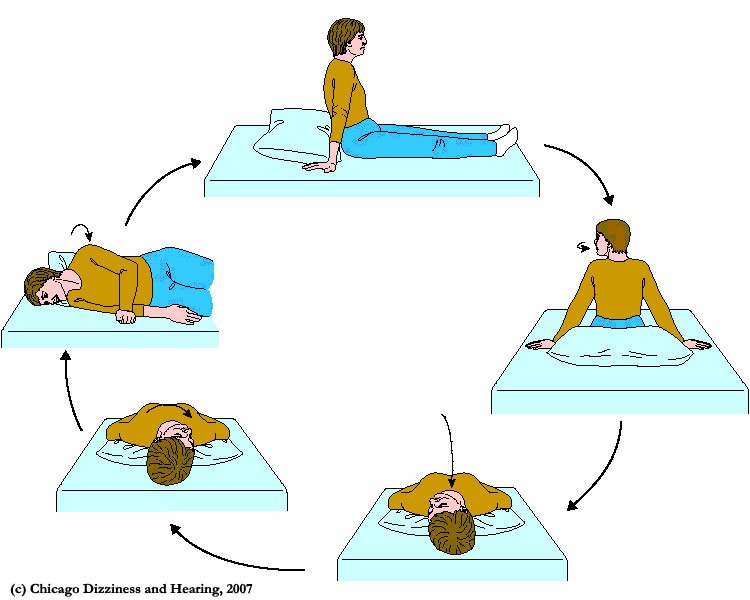
Epley Maneuver: Step 1
You will sit on the clinician’s exam table with your legs extended in front of you. The patient’s head will be turned 45 degrees to the affected side. Without changing your head position, the clinician will guide you back quickly so that your shoulders are on the table but your head is hanging over the edge of the table. In this position, the side of your head that is causing the worst vertigo is facing the floor. The clinician will hold you in this position for 30 seconds or until your vertigo stops.
Epley maneuver: Step 2
Then, without lifting up your head, the clinician will turn your head to look at the same angle to the opposite side, so that the other side of your head is now facing the floor. The clinician will hold you in this position for 30 seconds or until your vertigo stops.
Epley maneuver: Step 3
The clinician will help you roll in the same direction you are facing so that you are now lying on your side. (For example, if you are looking to your right, you will roll onto your right side.) The side that causes the worst vertigo should be facing up. You will be held in this position for another 30 seconds or until your vertigo stops.
Epley maneuver: Step 4
The clinician will then help you to sit back up with your legs hanging off the table on the same side that you were facing.
Treatment for lateral (horizontal) canal
This is a less common form of BPPV which can be treated with the Lempert maneuver also known as the log roll.
Begins by laying down with the head turned to the side of the affected ear being down. The patient then turns the head in 90 degree steps rolling on your back as the turning of the head happens. Every turn is held for 30 seconds. The maneuver is finished when the patient turns 360 degrees before sitting up.
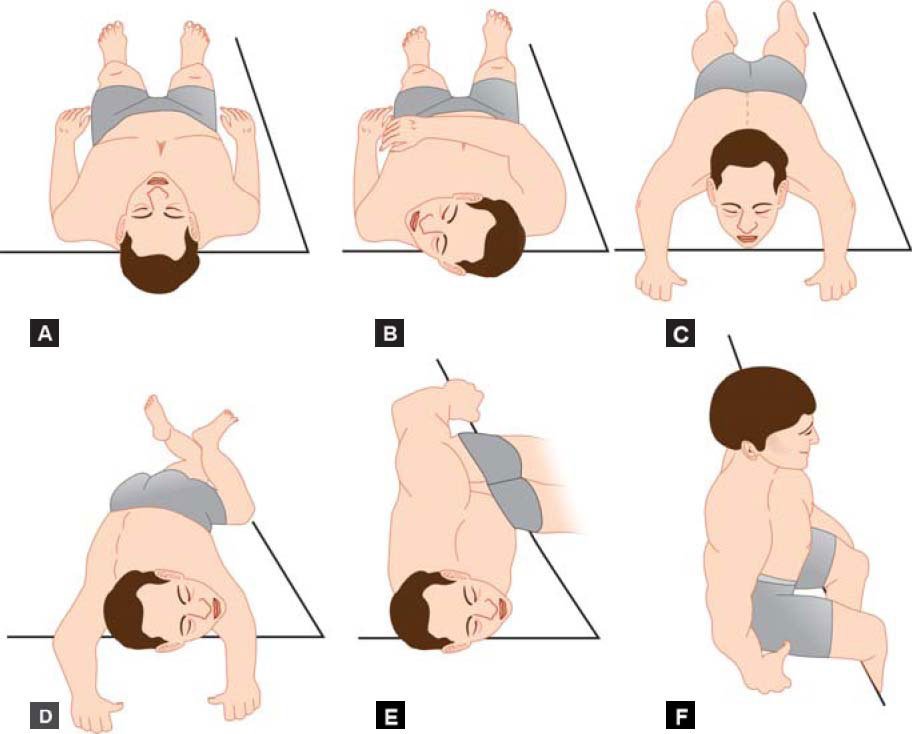
Treatment for superior canal
This is the least common form of BPPV using the Deep Head Hanging maneuver.
The patient is lying down on a clinician table with their legs extended. The patient’s head is tilted back by as close to a 90 degree angle as possible. After 30 seconds of this position the clinician bends the patient’s head forward to as close to 45 degrees as possible and held for 30 seconds before sitting up.

If you suspect you may have BPPV please contact our office so we can assist you.